Smoking ban health miracles
Earlier this year a paper was published in a peer reviewed journal that was so contrived and so flawed that I had hoped it would convince any doubters that the evidence for miraculous immediate health effects from smoking bans is entirely the figment of activist’s febrile imaginations. Sadly, it appears that I was wrong and that true believers including David Cameron still cling to the notion that smoking bans “have had a pretty dramatic health effect”. This delusion is shared by Anna Soubry who unforgivably and untruthfully claimed reductions in heart attacks and childhood asthma admissions as a result of the English smoking ban in evidence that she gave to the House of Lords (page 11). The fact that she was standing next to the less than impartial Andrew Black at the time is no excuse as only someone without interest in truth or reality would take anything Black says at face value.
The “growing body of peer reviewed evidence” used to justify these counter-intuitive claims is an indictment of public health industry ethics and medical journal standards. This recent contribution claiming a 12% reduction is asthma admissions as a result of the smoking ban originates from Imperial College London which is cause for further concern because Imperial is a top UK research establishment and as such charges young people a small fortune to be educated by what one would hope are top academics.
The culprits behind this affront to science are Stanton Glantz and Christopher Millett. In case anyone is labouring under the illusion that these two are objective scientists, Glantz is a well-known anti-tobacco activist who together with Millett holds extreme views on smoking in movies. Glantz was recently mentioned in the US congress in relation to a $680,000 grant that he used to make the bizarre claim that the Tea Party was created 25 years ago by big tobacco. It is extraordinary that we ban tobacco company funded research on the basis of scientific objectivity but, by a widely accepted double standard, treat the output of blatantly biased activist obsessives as “scientific evidence” fit for Prime Ministers.
This paper is yet another example of torturing numbers to fit a theory. The authors produce a lot of complex statistical waffle to obscure the deception but their essentially simplistic claim can be illustrated using annual data for childhood asthma admissions from the same NHS source they use. In the figure below the blue bars are years pre-ban and the orange ones the year of the ban and one year later. The solid red line is a simple linear fit to the pre-ban data.

The claim that the ban reduced asthma admissions depends on showing that admissions rates were increasing pre-ban and that after the ban admissions were lower than predicted had that trend continued along the path illustrated by the dashed red line. Millett uses the period 2002-2007 to model the “rising trend” in admissions but the NHS data goes back further and if we use all the available data the “trend” changes somewhat.

Cherry picking time periods is a common deception practiced by the public health industry together with taking advantage of coincidental variations in data series that happen to fit a theory or policy.
Those desperate to believe might argue that I am being too simplistic in that the “experts” took a more sophisticated approach and used monthly data. A 12% fall in admissions should not need sophisticated techniques to be apparent but it is true that 2007-08, the year of the ban, saw a big fall in admissions compared to the previous year. However, a look at NHS data for monthly admissions covering three years around the ban serves only to illustrate how the second element of the trick works. 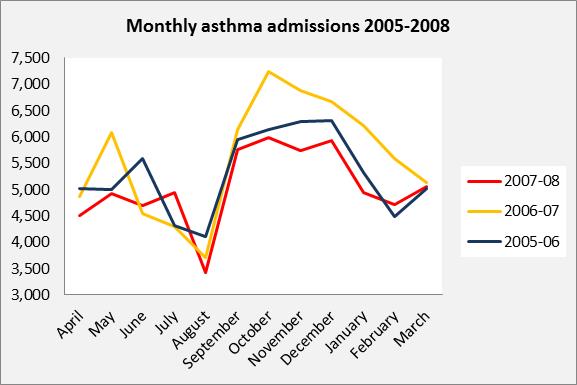
If I asked a group of seven year olds which of the lines on the chart above was the odd one out, I would expect the majority to say the orange one. The orange line represents monthly admissions for the year before the ban. We can align the data on the month of July which was when the ban came in but it makes little difference. Admissions were low in the year the ban came into force but not unusually so. Both the alleged upward trend before the ban and the apparent fall in the year it was enacted work for the activists only because peak season admissions were unusually high in the year before the ban. That stroke of fortune combined with the cherry picked time frame form the basis of the deception.
This peer reviewed paper appears to be nothing more than a cheap trick, an abuse of academic freedom for political purposes. The authors admit to some of its flaws but this did not prevent them from issuing a carefully worded press release that inevitably led to a misleading claim being widely broadcast by a gullible and uncritical media. It even made BBC TV news! This is not an isolated incident. It forms part of a body of highly publicised but fundamentally flawed “research” that has led some politicians and at least one national leader to erroneously believe in unlikely health miracles associated with interventions such as smoking bans. This might well influence opinions when reviewing existing or considering additional interventions, which one can argue is the main purpose behind such publications and their attendant publicity.
Of course, those politicians obsessed with public health are never slow to accept even the most unconvincing “evidence” if it suits their prejudices. Despite widespread incredulity over the facile “evidence” underpinning the implausible notion that smoking bans produce big falls in heart attacks, Sarah Wollaston of minimum alcohol pricing fame has claimed that the UK smoking ban:
“…was a very good example of evidence-based policy. If you look at what has happened in terms of deaths of cardiac disease, it has been staggering. There’s been a huge drop … It surprised even the health experts.”
Wollaston exhibits blind faith in “evidence” that is of no better standard than the article reviewed here. Her need to believe does not make it true, or a good basis for policy.
I have contacted Pediatrics and asked how something so obviously contrived as the Millett paper could survive peer review. I was informed that it was reviewed by people who are “experts in their field”. I wasn’t told what field, but expertise in either mathematics or ethics was apparently not considered necessary in this case. There are reasons why political stunts like this usually appear in medical journals rather than elsewhere in the literature and it is remarkable just how low some set the peer review bar. Peer review is supposed to be a minimum requirement able to identify fundamental methodological errors or false claims. Every time an article such as this is published in a “peer reviewed” journal, respect for this gold standard and science in general declines a little bit further. The collective damage is becoming significant and the implications extend way beyond smoking.
I have also contacted Imperial College press office but they have declined to comment on why they inflicted this press release on the general public. From direct experience I know that Imperial College employs many excellent lecturers and research scientists but based on this output I think that we should question what exactly young people are being taught for £9,000 a year and who is doing the teaching. Honesty, integrity and academic excellence are qualities that I would expect to see in those who benefit from the fees young people are now being asked to pay. I appear to be in a minority.
By Chris Oakley. Chris’ previous posts on Liberal Vision include: Minimum pricing – policy based evidence , Alcohol is Old News – Minimum Pricing for Digestives is the “Next Logical Step” , Soviet Style Alcohol Suppression Campaign Called for By Public Health Activists , Alcohol Taxation: The truth, the whole truth and nothing but the truth , Lies, damn lies, statistics &… , The Department of Health is Watching You! , New bounty on smokers helps GPs balance their books.
Tags: Anna Soubry, asthma, Christopher Millett, health miracles, Imperial College, smoking ban, Stanton Glantz
